Buruli Ulcer’s Global Presence
BACKGROUND
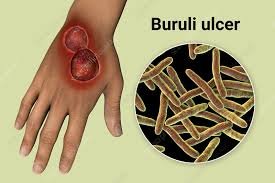
Buruli ulcer is a necrotizing cutaneous infection that is also called Bairnsdale ulcer, Daintree ulcer, Mossman ulcer, and Searl ulcer. It is caused by an infectious bacterium called Mycobacterium ulcerans, which produces a detrimental toxin responsible for skin damage. This disease is predominantly found in tropical regions, particularly in West Africa and Australia.
The inaugural record of Buruli ulcers can be traced to Sir Albert Cook, who conducted observations on afflicted individuals in Buruli County, Uganda. The etiological microorganism was effectively isolated by MacCallum in the year 1948 within the Bairnsdale region of Victoria, Australia. A resurgence in reported cases prompted the World Health Organization (WHO) to undertake a reclassification of Buruli Ulcer in 1998, categorizing it as a ‘neglected emerging infectious disease.’ Subsequently, this reclassification has stimulated persistent research endeavors in the realms of diagnosis, pathogenesis, and efficacious treatment modalities.
RELATED article: Buruli ulcer (Mycobacterium ulcerans infection)
Infections frequently result in the formation of ulcers on the arms or legs, which can damage skin or soft tissue. When left untreated, Buruli ulcers can lead to irreversible deformities and long-term health complications, including potential bone involvement.
It’s worth noting that the causative agent of Buruli Ulcer belongs to the same bacterial family as those responsible for tuberculosis and leprosy.
Signs and Symptoms
Due to the prolonged incubation period of Mycobacterium ulcerans, spanning from 1 to 9 months with an average of approximately 4.5 months, many patients encounter difficulty in identifying a specific initiating event. The initial lesions commonly manifest as solitary, painless dermal papules or subcutaneous nodules, occasionally accompanied by pruritus. The absence of pain in these early lesions frequently results in individuals postponing immediate medical attention. Suppuration and subsequent necrotic ulcer formation typically occur within 1 to 2 months. Patients generally maintain overall good health, and the occurrence of systemic symptoms such as fever or lymphadenopathy is rare, primarily ascribed to the immunosuppressive effects of mycolactone.
The peak incidence of cases typically occurs in March, particularly in swampy areas, suggesting an association with the rainy seasons in West Africa.
Signs and Symptoms
- Swelling of the skin
- Destroyed skin and soft tissue
- One or more slow growing, generally painless ulcers
- The initial indication of buruli ulcer typically presents as a painless lump, occasionally mistaken for an insect bite. This lump, medically termed a nodule, may occasionally be accompanied by itching and is commonly observed on the limbs, frequently near joints. Approximately 1 to 2 months later, the skin around the lump may commence deteriorating, leading to the development of an ulcer.
Physical Examination
In a typical presentation, Buruli Ulcers exhibit ulcerative expansion, with the potential to appear on any part of the body, although they are frequently observed on the lower extremities. Approximately 90% of these ulcers manifest on the limbs, with 60% specifically situated on the lower extremities. Nonulcerative lesions are detected in 0-30% of cases, while ulcerative lesions are evident in 70-100% of cases.
STAGES
In the preulcerative phase, Buruli ulcer initially appears as a solid, painless, subcutaneous nodule measuring 1-2 cm in diameter. Less common presentations include a dermal papule or an indurated plaque. In Australia, a more aggressive edematous variant is often observed. This variant, characterized by rapid and widespread swelling affecting an entire extremity, can progress into an extensive ulcer. Unfortunately, this presentation is frequently misdiagnosed as cellulitis.

The ulcerative phase manifests days to weeks later. The skin overlying the plaque or nodule gradually sheds, revealing an extensive necrotic ulcer with undermined edges. Subcutaneous necrosis may extend several centimeters beyond the ulcer’s edge, causing the lesion to appear smaller than its actual size. Characteristic features include a scalloped border and a sloughing, necrotic base. The ulcers may exhibit a yellow or green appearance and emit a characteristic odor. Pain and local lymphadenopathy indicate a potential secondary infection.
Buruli ulcers have the capacity to damage nerves, appendages, blood vessels, and may even invade bone. Metastatic lesions can arise in the skin, soft tissue, or bone through spread via the vasculature or lymphatics. Approximately 33% of patients present with underlying osteitis, osteomyelitis, or joint involvement. Intriguingly, one-fourth of patients with M. ulcerans osteomyelitis lack an apparent history of cutaneous Buruli ulcer. Half of these patients experience debilitating sequelae.
The healing process is gradual and may lead to cosmetically disfiguring scars and functional impairments if treatment is delayed
FOR MORE ARTICLES From Sandflies to Scars Investigating Leishmaniasis in the US
How Buruli Ulcers Are Transmitted
It is not known how people get Buruli ulcer,One possibility is that the disease is passed to humans by some insects that are found in water. While no proven link exists between human and animal infections, some animals can get the disease.
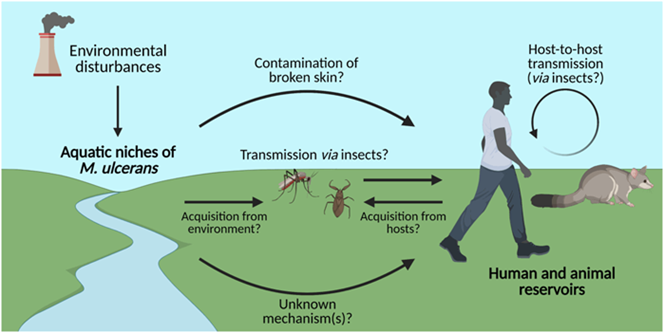
For example, laboratory tests from Victoria, Australia, confirmed the disease in several animals, including:
- Horses
- Dogs
- Alpacas
- Koalas
- Possums
PATHOPHYSIOLOGY
Mycobacterium ulcerans, a slow-growing species of mycobacteria, synthesizes a soluble polyketide exotoxin identified as mycolactone. This mycolactone possesses a distinctive capacity to extensively diffuse within subcutaneous tissue. What distinguishes mycolactone is its dual nature, characterized by both immunosuppressive and cytotoxic properties. This combination results in significant tissue damage without eliciting inflammation or the typical systemic symptoms such as fever, fatigue, or adenopathy. The discovery of mycolactone traces back to 1999, and ongoing research has elucidated its intricate mechanisms of action, as detailed below.

Epidemiology
In the United States, as of 2015, there have been no reported cases of Buruli Ulcer, according to information provided by the World Health Organization (WHO).
Globally, approximately 6,000 cases are reported each year, with the majority occurring in rural areas of Africa. Buruli Ulcer has been identified in 33 countries, with central and western African nations such as Côte d’Ivoire, Benin, Ghana, Democratic Republic of the Congo, Cameroon, Nigeria, Togo, and Liberia exhibiting the highest endemicity. Other affected regions include Australia, Papua New Guinea, Japan, and isolated cases in Central and South America. Notably, subtropical and swampy terrains are significant endemic areas for Mycobacterium ulcerans.
Race
There is no known racial predisposition to the disease.
Sex
No discernible differences in infection rates exist between males and females.
Age
Buruli Ulcer can affect individuals of any age, with the majority of cases occurring in children aged 5–15 years, except in Australia, where it is more prevalent in adults aged over 50 years
TREATMENT
“Effective treatment of Buruli ulcers typically involves a prolonged regimen of antibiotics and surgical debridement. Early detection and timely intervention are crucial since the resulting healing process often leads to scarring, which can pose a significant burden on patients in terms of morbidity.
RELATED ARTICLE Treatment of Buruli Ulcer
For detailed guidance on treatment, healthcare professionals and interested individuals can refer to the World Health Organization’s (WHO) publication titled ‘Treatment of Mycobacterium Ulcerans Disease (Buruli Ulcer).’ Recent research suggests that the recommended treatment now involves the combination of rifampicin (10 mg/kg once daily) and clarithromycin (7.5 mg/kg twice daily).”
If these antibiotics are not given soon after getting sick, the disease can sometimes lead to
- Deformity
- Functional disability (such as limited joint movement)
- Bone infection
- Secondary bacterial infection of skin ulcer lesions
Successful treatment of Buruli ulcers hinges on prompt and precise diagnoses. In cases where early intervention is possible, antibiotics alone are typically sufficient. However, when treatment is delayed, it may necessitate surgical debridement, the application of skin grafts, comprehensive wound care, and physical therapy to mitigate the development of debilitating complications.”
Prognosis
The outlook for Buruli Ulcer patients is generally positive, with most individuals achieving complete healing, sometimes with minor scarring or impairment. Hospitalizations, averaging around 3 months, are often necessary, even with medical and surgical care. The most favorable prognosis is associated with early treatment, ideally initiated before substantial tissue damage occurs.
In the absence of medical intervention, over half of those affected may experience functional limitations, with disfiguring scarring that can have a considerable emotional and socioeconomic impact. However, it’s important to note that treatment can be challenging in endemic areas where resources such as long hospital stays, antibiotic regimens, and surgical procedures are limited.
While Buruli Ulcer carries a low mortality rate, it imposes a significant burden in terms of morbidity and socioeconomic challenges. Skin and soft-tissue damage can extend extensively, involving up to 15% of the patient’s skin surface and potentially affecting deeper layers, including fascia, muscle, and bone.
Early identification and appropriate treatment are pivotal for a positive prognosis. Research by Klis et al indicated that 85% of patients with small lesions, receiving an 8-week course of antibiotics, reported no or minimal long-term impact on their quality of life. The Dermatology Life Quality Index median score was 0 (range, 0-4), signifying a good quality of life. These findings underscore the significance of timely intervention in contrast to the debilitating scars that may result if treatment is delayed.
Most systemic complications associated with Buruli ulcer arise from the side effects of prolonged antibiotic use, as discussed in the Treatment/Complications section.
Elderly patients tend to experience more severe disease and heightened treatment-related complications.”
Differential Diagnoses
- Cellulitis
- Cutaneous Squamous Cell Carcinoma
- Dermatologic Aspects of Actinomycosis
- Dermatologic Manifestations of Leprosy
- Herpes Zoster
- Kaposi Sarcoma
- Leishmaniasis
- Pyoderma Gangrenosum
- Ulcers Related to Sickle Cell Disease
- Snakebite
- Tuberculosis (TB)
- Venous Stasis Ulcer
- Yaws
